
Deadlier vaccines deployed in nine US states caused second death wave 4-6 months after jab: Paardekooper
Later death surge among vaccinated people in states along Interstate 75 indicates delivery route for slow-kill shots, claims VAERS researcher (Updated 5/9/22)

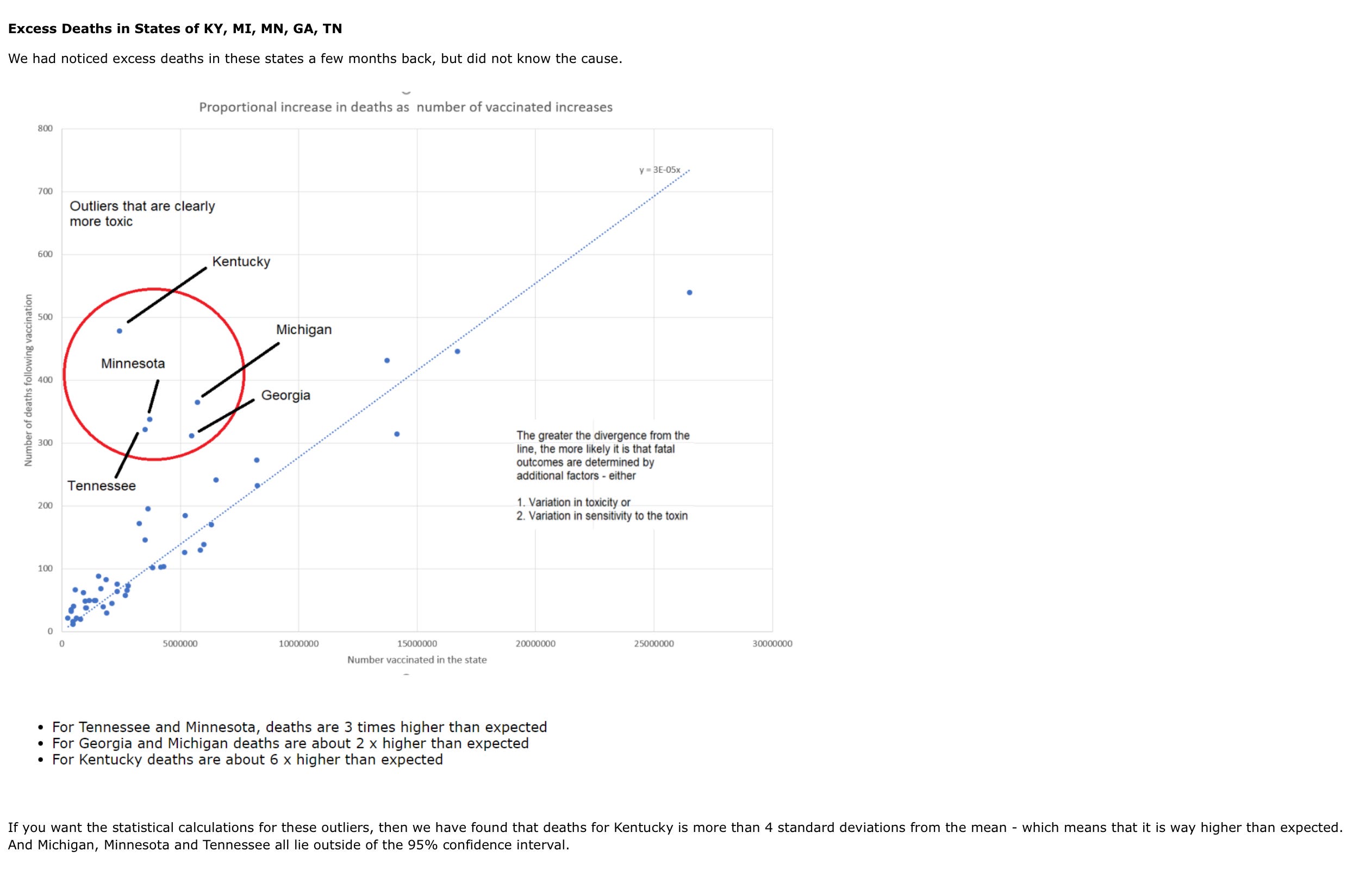
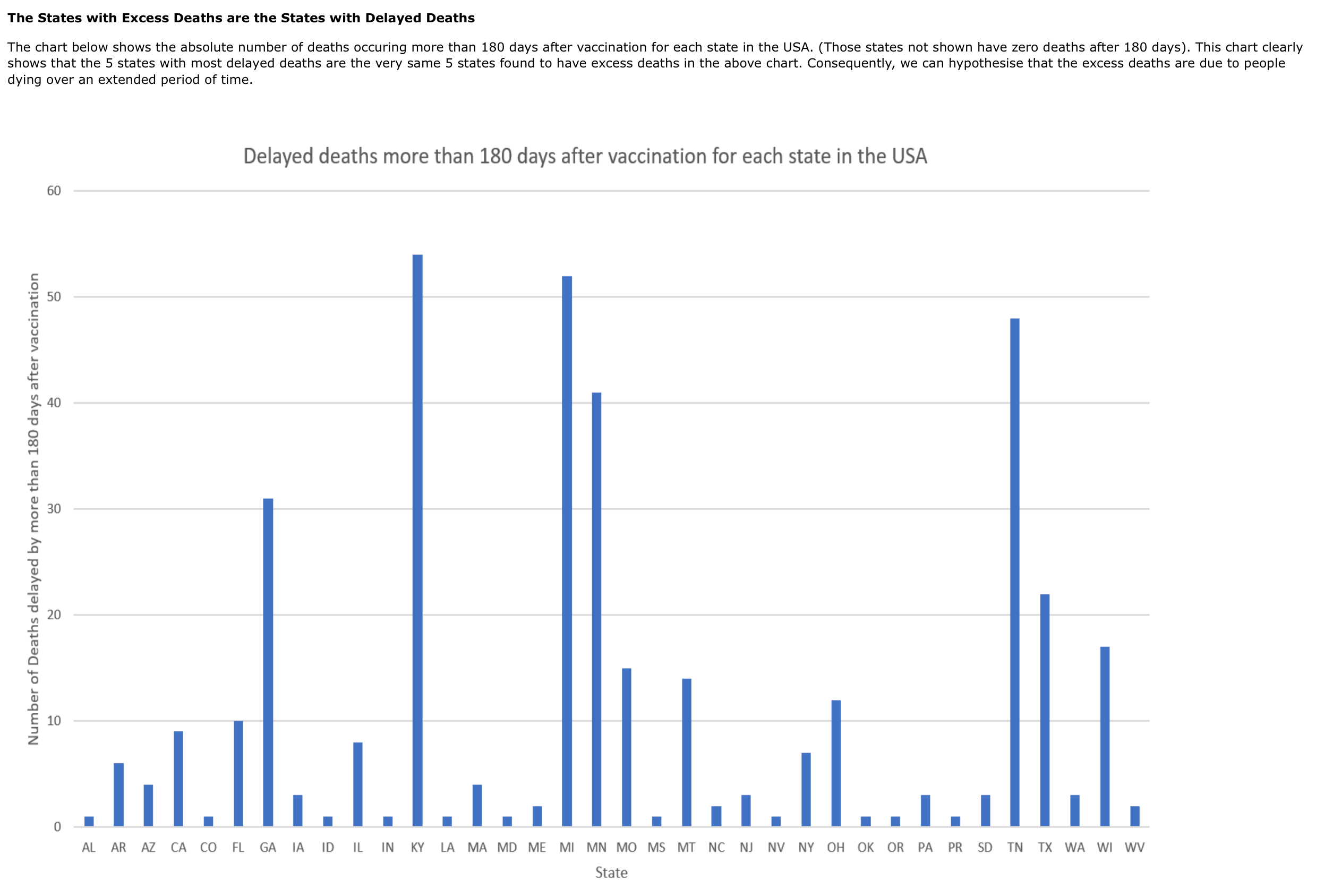
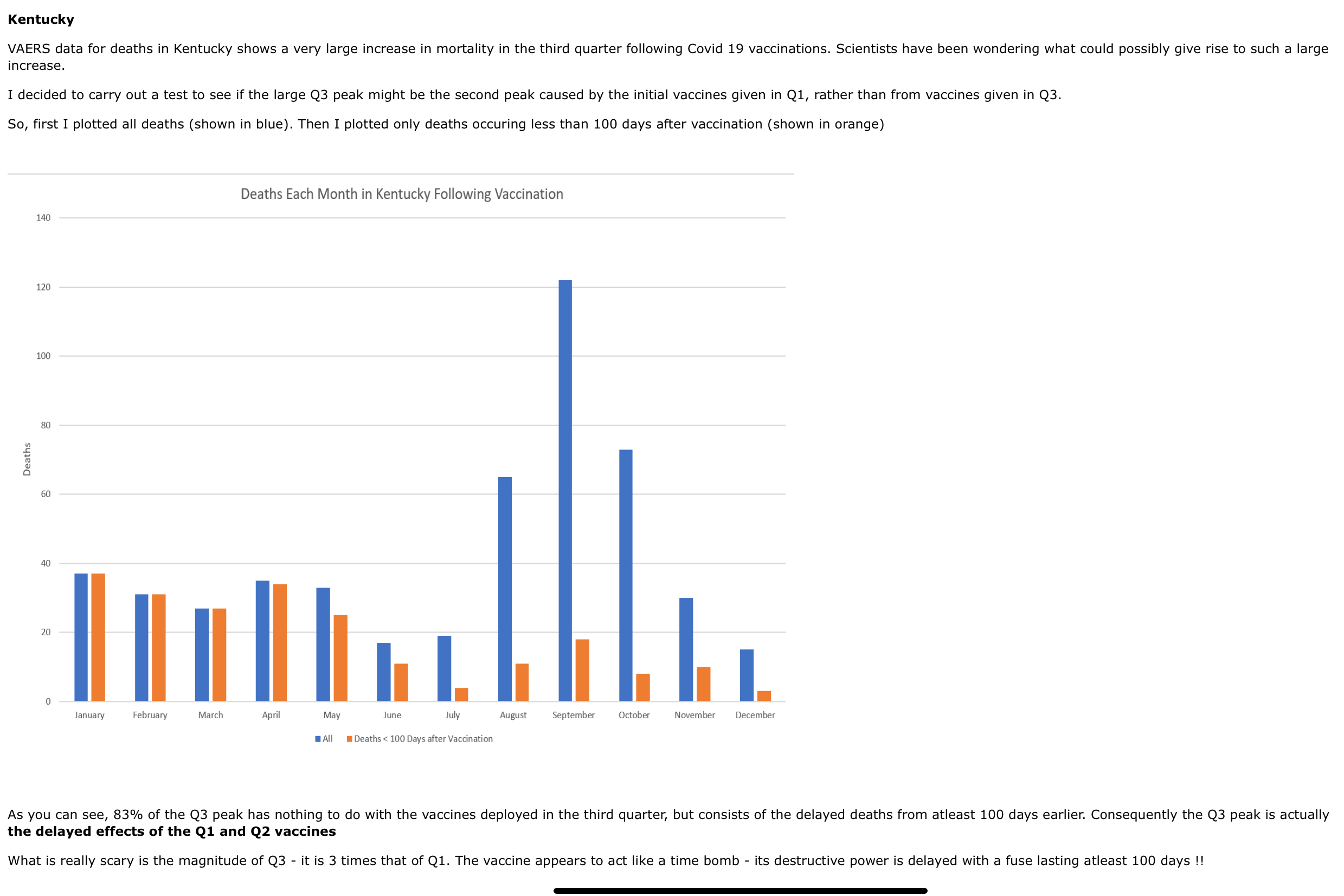
Researcher Craig Paardekooper says VAERS data show Covid-19 vaccines administered in the first two quarters of 2021 in nine US states states — Florida, Texas, Ohio, Wisconsin, and especially Michigan, Minnesota, Tennessee, Kentucky (most affected), and Georgia — produced not only an immediate spike in deaths during the first 30 days after vaccination, as occurred in all states, but also a second spike in deaths about 100 to 180 days after vaccination.
The other 41 US states experienced only the first (30-day) spike in deaths, not the second.
In his video The Mortality Bomb and related article The Second Peak, Paardekooper attributes the delayed deaths to some vaccines intentionally made more harmful than others.
Paardekooper:
It is incredible that many states do not show this delayed effect - the only explanation I can think of is that the vaccines may have been adulterated to test this delayed effect in select states, and on a younger age range.
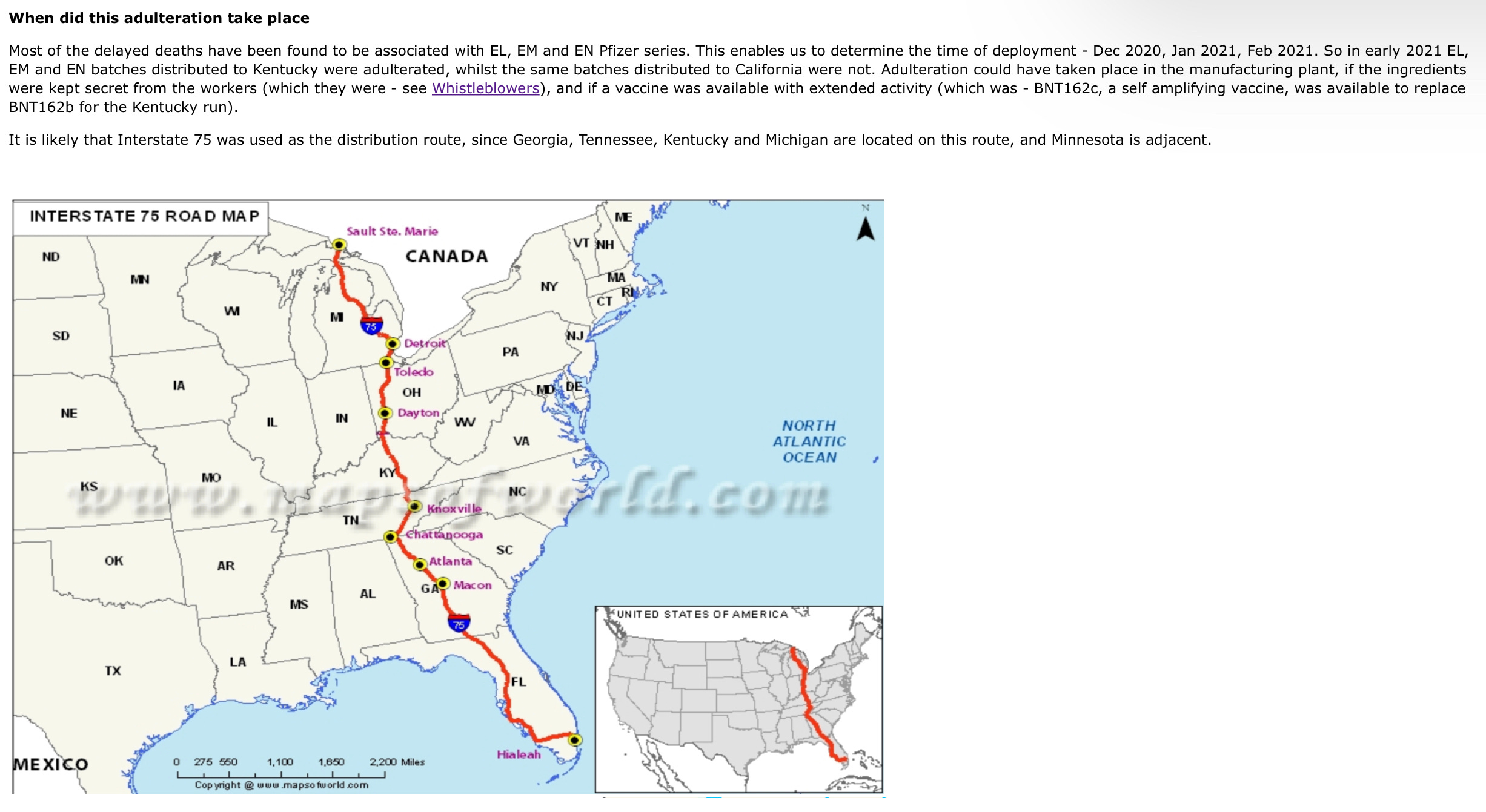
He further reasons at least some of these “hot” vaccines were likely delivered via US Interstate 75, as five affected states lie along the highway (Georgia, Tennessee, Kentucky, and Michigan) or adjacent to it (Minnesota).
The leading cause of death listed in VAERS during the first wave (up to 30 days after vaccination) was cardiac arrest.
During the second wave (4-6 months after vaccination), the leading listed cause of death was Covid-19.
If Paardekooper’s insights are correct, they imply that some particularly harmful vaccines:
suppressed immunity more than did unaffected Covid vaccines, making vaccinees more susceptible to Covid months after vaccination; and/or
kept cellular production of the viral spike protein or another toxin in jab recipients going longer, or at a higher rate, than did the other vaccines, and cumulative harm from this over months resulted in deaths attributed to Covid in many cases.
State death numbers not normalized to populations
One criticism of Paardekooper’s delayed-deaths analysis is the VAERS state death numbers he uses are apparently not normalized, i.e., they are not divided by the total number of people living, vaccinated, infected, or symptomatic with Covid in respective states.
So we don’t currently know states’ per capita delayed death rates or whether, for instance, Texas’s six-month postjab death rate was higher than Wisconsin’s, given that Texas is more populous than Wisconsin.
Nevertheless, Paardekooper’s findings appear valid and important for at least the following reasons:
Regardless of death rates, a large surge in absolute numbers of deaths 4-6 months after vaccination in some states but not others is significant and apparently not explained by different Covid infection rates in those states.
The three states with the highest 180-day postjab death numbers — Kentucky, Michigan, and Tennessee — have smaller populations than California and New York, for example, which exhibited many fewer excess 180-day deaths following vaccination.
So the higher death numbers seen in some states are not attributable to larger populations in those states.
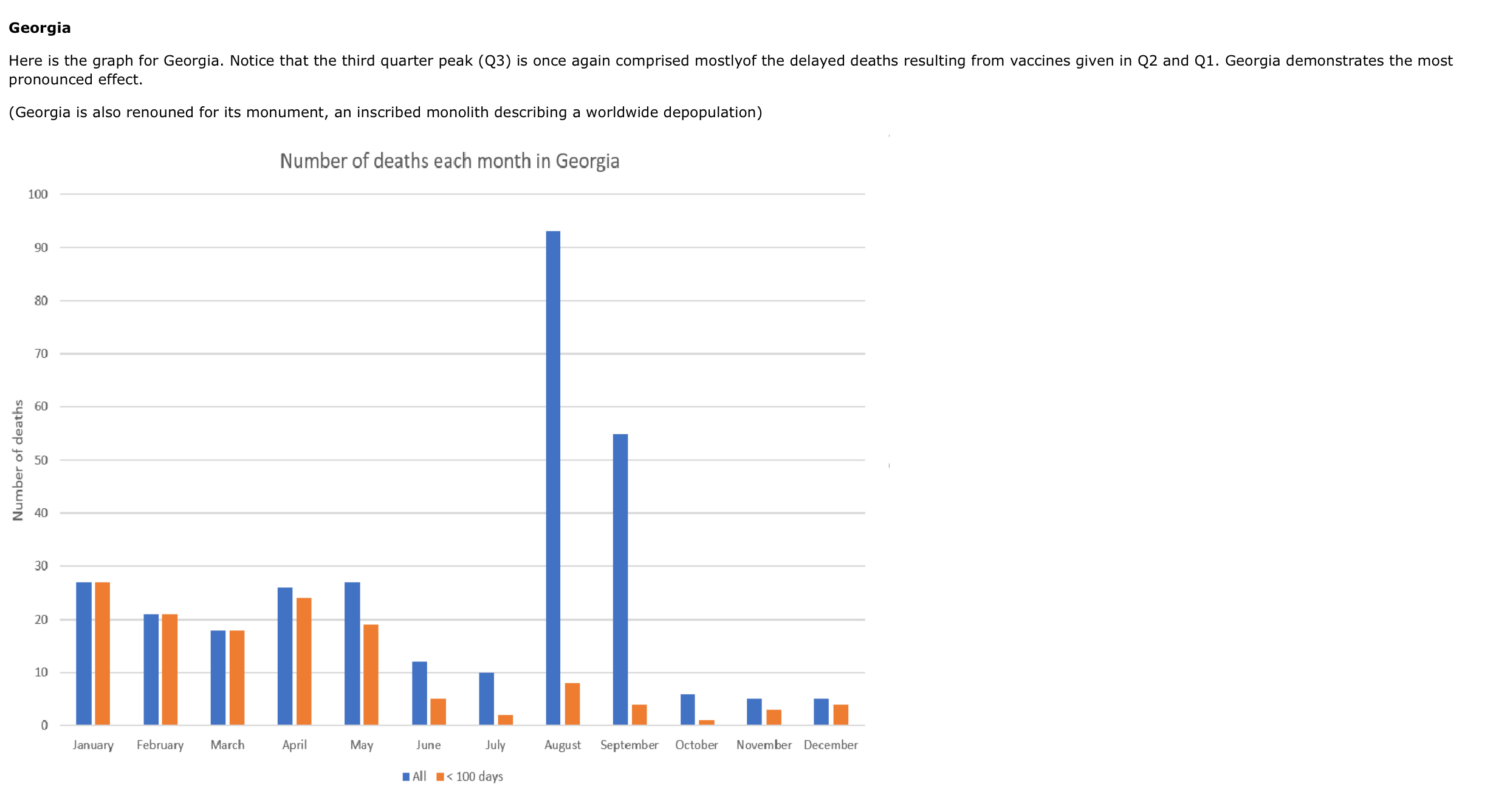
Exemplary graphs, for Kentucky and Georgia:
Thank you. Great article & DATA presentation. Chilling on so many levels.Supportive of so many individual experience people have been reporting all over the word. I have 4 close friends in different European countries and sadly they observed the same trend in their social circles after vaccinations. Its like "data" was being presented to people so much earlier than what we are seeing in charts now, if they only looked around with an open mind and observed what was going on in their social circles. Mindblowing.
EM exposure biologic damage stunningly similar to ‘covid’ / ‘injectables’...
was ‘covid’ introduced to obscure the biologic effects as EM exposures are ratcheted up with rollout of 5G into meta verse?
do certain formulations of the injectables exacerbate EM biologic damage? will the ‘injectables’ aid in the connectivity of the meta verse?
would explain the ‘necessity’ of endemic ‘covid’ and the ‘necessity’ of increasingly virulent variants.
statistical analyses don’t seem to control for EM exposures.
a lot of questions... certain that someone with a lot to gain knows the answers.